Last Thursday we had our all-day appointment at U of M. We weren’t sure what to expect but hoped to come away with a better understanding of the process we are going through and the facility that will become our second home. It didn’t take too long to get there – about 1.5 hours – but I can easily see how construction, traffic, or an accident could significantly change that timeframe. I-94 is not fun or commuter friendly.
Last Thursday we had our all-day appointment at U of M. We weren’t sure what to expect but hoped to come away with a better understanding of the process we are going through and the facility that will become our second home. It didn’t take too long to get there – about 1.5 hours – but I can easily see how construction, traffic, or an accident could significantly change that timeframe. I-94 is not fun or commuter friendly.
The hospital was easy enough to find, and you have to pay for parking which I think stinks considering we’ll be spending how much money for services there?? I mean it is cheap (if you don’t lose your ticket…) Unfortunately we will not be in the new women and children’s hospital, but we should be over there for his other surgeries. Too bad, because it looks and sounds lovely. The old hospital… well… let’s just say the conditions don’t exactly match the caliber of care provided there.
8:00 am – Cardiologist appointment
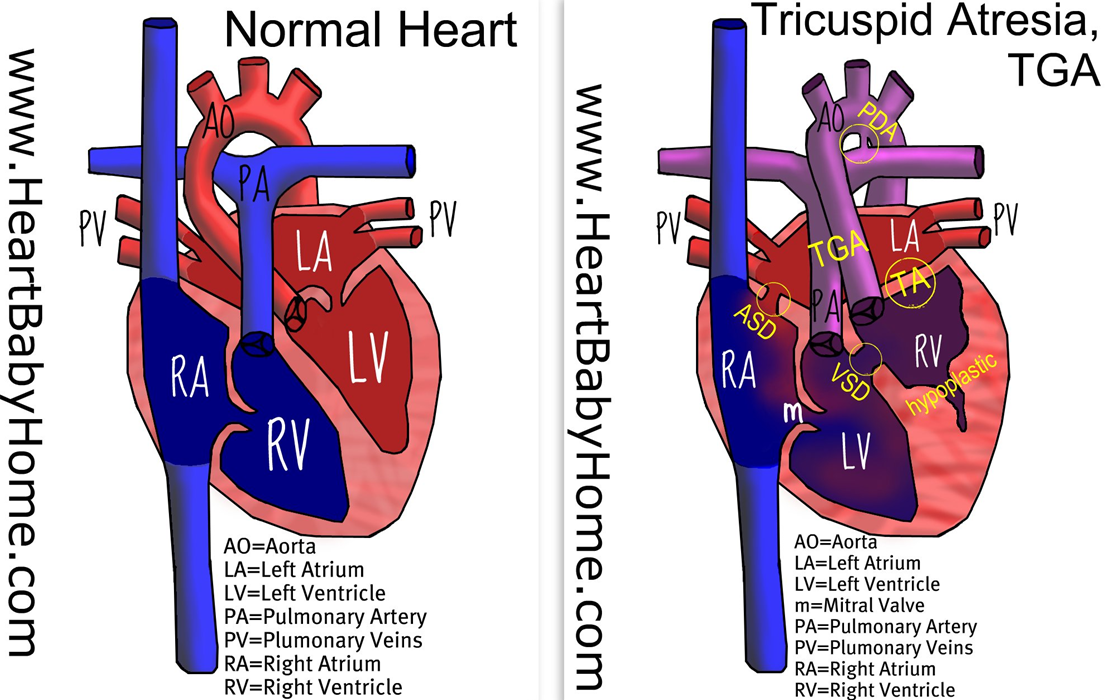
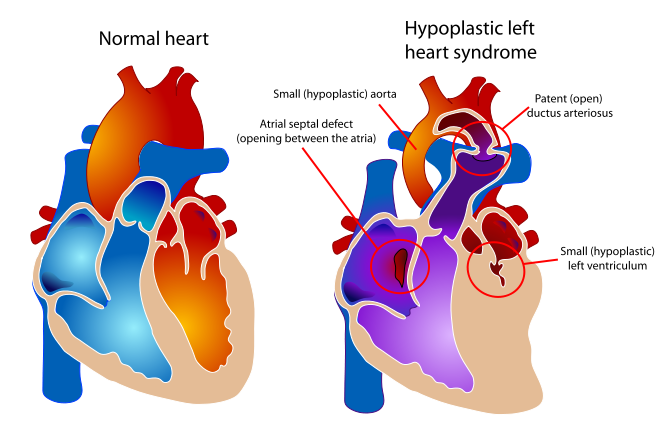
Our first appointment was to receive our second echocardiogram at the Pediatric Cardiology center in Mott Children’s Hospital. We got to meet with Kathy, one of the nurses and the one who would help guide us through our day. I was especially looking forward to this appointment as previously there was a slight discrepancy in what his condition might actually be, and this was an opportunity to have another expert provide their opinion. The tech was very thorough, albeit a bit fidgity and fussy at times, probably due to a lack of angle cooperation by baby tricky. We met with Dr. Russell who confirmed the diagnosis of Dr. Fountain-Dommer. He actually gave her some kudos and spoke very well of her for catching this different condition and not going along with the suspected condition of HLHS. We asked him to point out some structures on the echo and he happily answered all of our questions.
What we learned:
- UofM sees about 50-60 single-ventricle cases a year, so about 1 a week. About 30 are HLHS. There are a decent amount of TA cases, TA/l-TGA is still rarely seen.
- The first surgery, the Norwood procedure, will happen within the first week of life
- If we need to have any specialized equipment at home, it might be a feeding pump. Hopefully he will pick up feeding, but if needed he will continue to be tube fed. They will teach us CPR and how to insert his tube before we are discharged.
- At minimum, Evan will be on baby aspirin and diuretics – hopefully that will be it!
9:30 – OB/GYN appointment
We shuffled off to the Taubmann center for our next appointment. I had no idea really what this appointment was for, other than to load my information into the database. We did come prepared with questions, particularly because we felt that these were the individuals who would be able to give us the best birthing information. We met with Dr. Mozurkewich and again she answered all of our questions. We also talked with a nurse who gave us information on the 3rd trimester as well as a pretty nice birthing book. most of our time in this appointment was spent waiting, but that was ok because we could go over the info received at the cardio appointment.
What we learned:
- Cesarian births are not encouraged, and there is a strong leaning toward natural childbirth (I use natural to mean vaginal). The thinking is that 1) he is still connected to me until they cut the cord so he should be ok 2) the compression of giving birth helps to free fluids from the lungs and promote circulation. Obviously if a c-section is needed it is done, but they encourage one to try.
- Whether we induce or not depends on personal preferences and the opinions of the cardiology group. They do not see harm in waiting for nature to take its course. First babies usually take a little while, so even the drive from Kzoo does not make them lean one way or another.
- Whomever is on call will be delivering, so we might meet the particular doctor before hand or maybe just that day
- I will deliver in an operating room (more detail about that later)
- Episiotomies are not commonly performed
- If I want to have a medicine-free birth, that’s ok. They will probably add an IV port just in case
- With a natural birth, as many people as I want (realistically) can be in the room. With a c-section, only Will would be in the room with me
- I’m glad we brought a backpack to hold all of our paperwork!
11:00 – Social Worker appointment
We were supposed to meet with our surgeon next, but since we were meeting her between surgeries, we needed to be a bit flexible with our time. We went back to the Pediatric Cardiology center, paged Kathy the nurse, and she got a hold of Barb, a social worker with the department of pediatric cardiology. She has worked there for 22 years and holds a wealth of information
What we learned:
- If we want to have him baptized, blessed, or christened before surgery we can do so. The hospital chaplains can provide the services or we can have our own person come in. Just thinking of it makes me cry but something we will want to do.
- We will deliver in the high-risk side of the Woman’s East birthing center. We will do the great deal of our labor in the room, and when the time comes to get the show on the road, I will be wheeled down the hall (~100 ft or so?) to an operating room. It doesn’t really look like an operating room like you see on TV, but it is more important that adjacent to the room there is a newborn crash room. It holds every kind of equipment they might need in case something goes wrong. He will be whisked away into there after birth and if he’s pink and breathing ok, they will bring him back to be with us for a few minutes. Hopefully this is the case because it is extraordinarily important to me to get pictures of him with no scar and not hooked up to anything. Evan will have tubes and wires for the next 4-5 weeks, so images of him looking like every other normal baby will be awesome.
- He will spend the next week-ish (until his surgery) in the NICU. Hopefully he will be a big ole fat turkey baby and will look out of place next to those skinny babies. We pray that his breathing will be ok and he won’t need to be on a ventilator, because if he is, then we won’t be able to hold him. And I don’t know about you but not being able to hold your new baby is not something I am prepared to deal with.
- There are 40 NICU beds (10 beds in 4 rooms) and only 2 people can be bedside at a time. Anyone can visit but they MUST be healthy.
- While in the NICU, we can bring something that smells like us but most comforting to him would be recordings of our voices, like if we read books to him. That is the sense he is most used to at that point.
- Surgery will be on the 5th floor and afterward he will stay in the cardiac NICU which only has 15 beds but is specifically monitored by cardiologists. He’ll be there 1-2 weeks I am thinking. 100% of babies are on ventilators after surgery, so we will only be able to touch his little hands and such. This might not be a bad thing because I am not sure I would want to hold him because he will be so delicate. Sometimes the chest is left open and there are quite a few tubes to drain fluid. Here is an image of a Facebook friend’s little baby after this surgery and we would anticipate Evan to look pretty similar. Warning – it is a little tough to look at. And double warning – this is the sweet little baby that passed away and I mentioned in a previous post, so don’t read the blog if you don’t want to cry.
- Once he is off the vent and tubes start to come out, he can transition back to the NICU or bypass that entirely and go to the general care recovery rooms. While in these rooms, we’ll be able to do real parent things like change diapers and feed him. Gasp! He will have been tube fed up to this point and then it is on to bottles and then breastfeeding. Bottles are easier on weaker babies, so they like to start with those. He will be staying in the room and there is a larger bed for parents to stay in too. They encourage parents to stay in the room by switching on and off. Here we will learn CPR, how to put in his feeding tube, and how to take care of his wounds. We’ll be there for about 2 weeks and can then go home. Yay!
- He will have his “little boy” procedure after his surgery, while in the general care room. Like he doesn’t have enough problems already, right? Poor fella…
- They have pumping rooms and freezer storage system to keep track of everything so we can make sure Evan gets the most nutrition, even if he gets it via tube
- We may be eligible for Children’s Special Healthcare Services or 30-day Medicaid services as well
- Mott is billed under the U of M health system
11:45 – Meeting with the surgeon
This occurred during our conversation with Barb as the doctor became available. Her name is Dr. Jennifer Hirsch and she looks way young (we guestimate she should be ~42ish but easily looks 10 yrs younger), is very beautiful (her official doctor pic does not do her justice), very smart (she went to Harvard people), and was extremely kind and open to talk to. She was the first person at U of M to ask if our son had a name and referred to him as Evan when talking about him. Evan will die without any surgical intervention so it was surreal to meet the person who is going to save his life. We cried after she left. It is a bit overwhelming.
Things we learned:
- 75% of babies will live to have the 2nd surgery at 4-6 months. Not that this was new info, but it confirmed some of the numbers we had read about online.
- The timing of the 2nd surgery will depend on how fast he is growing. In the 1st surgery, they will put a BT shunt to reduce bloodflow to his lungs (otherwise too much would go there and not enough would go to the body). They have to guesstimate the shunt size, and essentially when he outgrows this is when he has the 2nd surgery. If born on July 17, that would give a November-January timeframe. I’m not excited about it being holiday season and illness season to have open-heart surgery. It also makes it trickier to know when to take time off of work, but we’ll just have to play it by ear.
- For the 2nd surgery, they detach the superior vena cava and attach it passively to the pulmonary artery (this is the big vein coming from the head/arm/upper body region). They do this one first (instead of the inferior vena cava which is the big vein returning from the lower body) because babies are all head and it will provide the most relief for the heart. Once kids become mobile and start to use their lower bodies more (18-36 months old) then they have the 3rd surgery to attach the body vein passively to the pulmonary arteries.
- Evan will be cyanotic until the 3rd surgery (blood oxygen level below 90%) but will look like kids when they get out of the bath – a little blue to the lips and fingertips.
- She gave us her email and encouraged us to send her any questions or comments we might have
After this we hauled ass to go get something to eat. It’s like they didn’t schedule a time for this or something… very weird…
1:30 – Genetic Counseling appointment
We had to have this appointment even though we received genetic counseling at Bronson. It’s just part of the packaged deal. This was at the Perinatal Assessment Center also in Mott. It was nice to be able to talk to someone again if we did have questions. They offered an amnio again and we declined. Given that no other health issues have come up on ultrasounds we feel the likelihood of him having any genetic condition to be low.
2:30 – Ultrasound appointment
Yay more pictures of baby boy! The tech was lovely and from Kzoo. She said everything was looking good except he was being a little uncooperative and tricky. Afterward, we met with Dr. Treadwell and she confirmed that she did not have any concerns for any other conditions to be present. A nurse, Liz, gave us a tour after the US and showed us the birthing areas and NICU on the 4th floor. It was very nice of her to take the time to help us get a sense of things, although I think we will want a more general tour too in the future.
What we learned:
- Evan weighs about 3 lbs@ 28 weeks, putting him in the 59th percentile. Definitely thought he would be bigger but I think he will have plenty of time to get huuuge.
- Evan is very limber. He was sitting breech, I think footlong breech, because he was holding one foot right up to his face. I’m not sure where the other one was?
We are going to go back June 10th for another cardio, OB, and ultrasound appointment. Until then, we have our regular appointment at Bronson in a couple weeks. We will probably go to U of M 1 more time after that prior to delivery, but otherwise we’ll just do some co-care with Bronson.
Here is a profile. I guess that is some brain development, so that looks cool. The smudge by his face is a foot I think.

This is the foot that kept getting in the way!

They tried to do a 3-D image but of course it looks all crazy. I only share because I love those toes! The other smudge by his face must be an arm or something.

 We had our second appointment at the University of Michigan on June 10th. This appointment put little Evan at 34 weeks and 5 days.
We had our second appointment at the University of Michigan on June 10th. This appointment put little Evan at 34 weeks and 5 days.